The majority of Americans will be affected by back pain at some time in their lives. Dr. Shane Burch explores the spine and discusses the causes and management of back pain. Series: UCSF Mini Medical School for the Public [8/2010] [Health and Medicine] [Show ID: 18539]
Sonntag, Oktober 31, 2010
Samstag, Oktober 30, 2010
Botox for Migraine
http://www.relieve-migraine-headache.com/botox-for-migraine.html
发自我的 iPhone
欧洲也才批准了Botox注射治疗偏头痛。
十分可笑的是注射部位,那不是对传统的偏头痛理论的颠覆?
是的,应该颠覆。
以我在德国5年的治疗方法,这个注射也是要被颠覆的。
因为,我从来就是在后方治疗,而80%的患者前额和眼部的症状消失。那些症状无非是一些牵涉痛,反射痛罢了。
Botox for Migraine
Over the past few years, there has been increased interest in using Botox for migraine. Some people feel it has been an almost miraculous solution for them. But the trials and research hasn't always been convincing. Is Botox for migraines something you should try?
A little background on Botox
Botox is botulinum toxin, a toxin produced by bacteria. It's actually extremely poisonous, and often is ingested as a result of not handling and cooking meat properly (botulism is often fatal).
But botulinum toxin A (Botox) has become famous for it's other application - getting rid of wrinkles. The treatment was discovered in Canada in 1987 by Jean and Alastair Carruthers, and since then brand names Botox, Neurobloc and Myobloc (botulinum toxin B) have been used (in very small doses) to decrease wrinkles and frown lines.
But the next discovery was that patients with migraine found their attacks to be decreasing when they had Botox treatment. Why was this happening? Was it just a coincidence?
Since then, research has begun to try to understand why it works, and when it works, and how Botox for migraine might best be used.
How does it work?
In your body, a chemical (neurotransmitter) known as acetylcholine sends signals for muscles to contract. Botox as a toxin binds the nerve endings, blocking the release of the chemical. Essentially, your muscles don't get the message to contract, and so they relax. In a proper treatment, the muscles won't contract (causing wrinkles), but will still have enough strength for normal use.
Why it may work to relieve migraine is not certain. Could it just be that relaxing certain muscles slows the migraine chain reaction? It's more likely that it blocks pain signals, or may even block signals that contribute to the migraine.
An article at the Mayo Clinic simply says,"the drug may cause changes in your nervous system that modify your tendency to develop migraines".
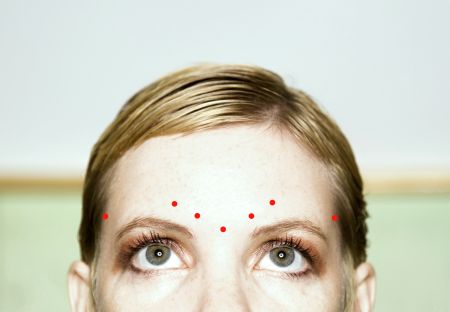
Botox injected in the forehead for migraines
Botox for migraine - injections
So just how is Botox for migraines used? Well, one way is through simple injections. The treatment is given in a series of shots. Some patients have found almost immediate relief. But the interesting thing is that the improvement tends to last for several months.
The injections may be expensive. Many patients need to weigh the cost against the amount of improvement they receive and the length of time the injections seem to help for. It's important to discuss the option with your doctor and keep a headache diary.
Neither are all injections created equal. Sometimes injections are simply done in a band-like fashion around the skull. But as our understanding increases about what works, different approaches, more specific approaches are being taken.
For example, Dr Jeffrey E. Janis advocates finding "peripheral trigger points", using them as a roadmap to use Botox for migraine.
Read more here about what Botox headache injections are like.
Botox and surgery
Dr. Janis' believes that this process can go even farther. The newer idea is that the Botox injections can find those trigger points - and then surgery can do the rest.
Instead of using a shotgun approach - simply injecting everyone the same way - some researchers believe that you can use the injections as a test. Which muscles are triggering the migraine attacks? If those specific muscles can be found, surgery can keep the problem from resurfacing in the future.
Dr Janis explains: "It's like a math equation. I will inject the Botox into one trigger point at a time and leave the others alone. The Botox is used as a diagnostic test to determine what trigger point is causing the problem. If patients get a benefit from the Botox, they likely will get a benefit from the surgery. If there's no benefit from the Botox, then there won't be a benefit from the surgery."
This treatment has some very controversial aspects. Of course, most are sceptical that migraine can be relieved by focusing on muscles. Though muscle problems may be a trigger, it's generally accepted that the migraine problem itself lies deep in the brain. Muscle issues may actually be a trigger in only a few migraine sufferers.
Still not ready for prime-time?
Groups like the American Academy of Neurology are not ready to accept Botox for migraine as a major treatment. In the spring of 2008, they suggested that Botox injections were no better than a placebo, based on the current evidence. (Read Botox Works on Muscle Disorders But Not Migraines) They recommended that this treatment not be suggested for people with episodic migraine and chronic tension-type headaches.
But wait - what about all these people that claim Botox has changed their lives, by relieving migraine? Well, the fact of the matter is that the research is still in its infancy. It seems that Botox treatments do work, for some. And for some they work very well.
But when compared against the many other treatments out there, the evidence still needs to be built up. In other words, there are many other things you can try, and probably should try, before you try Botox for migraine.
Some research is starting to suggest that patients with certain kinds of migraine pain may benefit most from Botox. That would explain why the more general studies don't show the same improvements. (Read this study on exploding vs imploding headache, for example, from 2007)
And different studies measure things differently. For example, what if Botox for migraines decreased the frequency of migraine attacks, but not the intensity?
If you are interested in trying Botox, take a look at some of the latest techniques, and discuss them with your doctor. Be sure you have a good idea what else is out there, and what the pros and cons are.
Read more about some of the earlier Botox for migraine studies here.
发自我的 iPhone
欧洲也才批准了Botox注射治疗偏头痛。
十分可笑的是注射部位,那不是对传统的偏头痛理论的颠覆?
是的,应该颠覆。
以我在德国5年的治疗方法,这个注射也是要被颠覆的。
因为,我从来就是在后方治疗,而80%的患者前额和眼部的症状消失。那些症状无非是一些牵涉痛,反射痛罢了。
Botox for Migraine
Over the past few years, there has been increased interest in using Botox for migraine. Some people feel it has been an almost miraculous solution for them. But the trials and research hasn't always been convincing. Is Botox for migraines something you should try?
A little background on Botox
Botox is botulinum toxin, a toxin produced by bacteria. It's actually extremely poisonous, and often is ingested as a result of not handling and cooking meat properly (botulism is often fatal).
But botulinum toxin A (Botox) has become famous for it's other application - getting rid of wrinkles. The treatment was discovered in Canada in 1987 by Jean and Alastair Carruthers, and since then brand names Botox, Neurobloc and Myobloc (botulinum toxin B) have been used (in very small doses) to decrease wrinkles and frown lines.
But the next discovery was that patients with migraine found their attacks to be decreasing when they had Botox treatment. Why was this happening? Was it just a coincidence?
Since then, research has begun to try to understand why it works, and when it works, and how Botox for migraine might best be used.
How does it work?
In your body, a chemical (neurotransmitter) known as acetylcholine sends signals for muscles to contract. Botox as a toxin binds the nerve endings, blocking the release of the chemical. Essentially, your muscles don't get the message to contract, and so they relax. In a proper treatment, the muscles won't contract (causing wrinkles), but will still have enough strength for normal use.
Why it may work to relieve migraine is not certain. Could it just be that relaxing certain muscles slows the migraine chain reaction? It's more likely that it blocks pain signals, or may even block signals that contribute to the migraine.
An article at the Mayo Clinic simply says,"the drug may cause changes in your nervous system that modify your tendency to develop migraines".
Botox injected in the forehead for migraines
Botox for migraine - injections
So just how is Botox for migraines used? Well, one way is through simple injections. The treatment is given in a series of shots. Some patients have found almost immediate relief. But the interesting thing is that the improvement tends to last for several months.
The injections may be expensive. Many patients need to weigh the cost against the amount of improvement they receive and the length of time the injections seem to help for. It's important to discuss the option with your doctor and keep a headache diary.
Neither are all injections created equal. Sometimes injections are simply done in a band-like fashion around the skull. But as our understanding increases about what works, different approaches, more specific approaches are being taken.
For example, Dr Jeffrey E. Janis advocates finding "peripheral trigger points", using them as a roadmap to use Botox for migraine.
Read more here about what Botox headache injections are like.
Botox and surgery
Dr. Janis' believes that this process can go even farther. The newer idea is that the Botox injections can find those trigger points - and then surgery can do the rest.
Instead of using a shotgun approach - simply injecting everyone the same way - some researchers believe that you can use the injections as a test. Which muscles are triggering the migraine attacks? If those specific muscles can be found, surgery can keep the problem from resurfacing in the future.
Dr Janis explains: "It's like a math equation. I will inject the Botox into one trigger point at a time and leave the others alone. The Botox is used as a diagnostic test to determine what trigger point is causing the problem. If patients get a benefit from the Botox, they likely will get a benefit from the surgery. If there's no benefit from the Botox, then there won't be a benefit from the surgery."
This treatment has some very controversial aspects. Of course, most are sceptical that migraine can be relieved by focusing on muscles. Though muscle problems may be a trigger, it's generally accepted that the migraine problem itself lies deep in the brain. Muscle issues may actually be a trigger in only a few migraine sufferers.
Still not ready for prime-time?
Groups like the American Academy of Neurology are not ready to accept Botox for migraine as a major treatment. In the spring of 2008, they suggested that Botox injections were no better than a placebo, based on the current evidence. (Read Botox Works on Muscle Disorders But Not Migraines) They recommended that this treatment not be suggested for people with episodic migraine and chronic tension-type headaches.
But wait - what about all these people that claim Botox has changed their lives, by relieving migraine? Well, the fact of the matter is that the research is still in its infancy. It seems that Botox treatments do work, for some. And for some they work very well.
But when compared against the many other treatments out there, the evidence still needs to be built up. In other words, there are many other things you can try, and probably should try, before you try Botox for migraine.
Some research is starting to suggest that patients with certain kinds of migraine pain may benefit most from Botox. That would explain why the more general studies don't show the same improvements. (Read this study on exploding vs imploding headache, for example, from 2007)
And different studies measure things differently. For example, what if Botox for migraines decreased the frequency of migraine attacks, but not the intensity?
If you are interested in trying Botox, take a look at some of the latest techniques, and discuss them with your doctor. Be sure you have a good idea what else is out there, and what the pros and cons are.
Read more about some of the earlier Botox for migraine studies here.
Freitag, Oktober 29, 2010
太极武当 / 有形无形 /德国科隆的设计师
晚上看到这个片子。当然亲切。武当山下就是我的家乡
居然要请德国科隆人为武当山设计建筑,看来我家乡的人越来越有国际大视野了。那个德国老先生竟然了解老子,年轻时有一本老子的口袋书,还带上战场。
节目最后,那个领导,似乎以前在茅箭区工作过吧。
居然要请德国科隆人为武当山设计建筑,看来我家乡的人越来越有国际大视野了。那个德国老先生竟然了解老子,年轻时有一本老子的口袋书,还带上战场。
节目最后,那个领导,似乎以前在茅箭区工作过吧。
Neues Gesicht, neues Leben, 新生活需要新面孔,看到他我很吃惊。
Quelle: http://www.20min.ch/wissen/gesundheit/story/16733474
Dallas Wiens Gesicht war durch einen Arbeitsunfall bis zur Unkenntlichkeit entstellt worden. Eine komplizierte Operation soll dem Amerikaner bald ein ein neues Antlitz schenken.
Er verfügt weder über Augen noch über eine Nase. An der Stelle, bei der in einem Gesicht der Mund zu finden ist, zeigt sich lediglich ein Schlitz ohne Lippen.
Dallas C. Wiens war ein ganz normaler Twen, bis sich sein Leben durch einen Unfall während der Ausübung seines Jobs drastisch veränderte: Er geriet an eine Hochspannungsleitung, die sein Gesicht vollständig verbrannte. Seither musste der 25-jährige Vater einer kleinen Tochter mehrere Hauttransplantationen über sich ergehen lassen - klassische Gesichtsmerkmale konnten dabei nicht wiederhergestellt werden, bisher: Dallas Wiens bekommt bald ein neues Aussehen - ihm wird ein komplettes Gesicht verpflanzt. (dga/rre)
<img src="http://20min.wemfbox.ch/cgi-bin/ivw/CP/iApp/iphoneapp/feed" width="1" height="1" border="0" />
<img src="http://20minde.wemfbox.ch/cgi-bin/ivw/CP/iApp/iphoneapp/feed" width="1" height="1" border="0" />
Von meinem iPhone gesendet
Donnerstag, Oktober 28, 2010
Montag, Oktober 25, 2010
Sonntag, Oktober 24, 2010
New treatments for Dupuytren contracture 注射用XIAFLEX(collagenase clostridium histolyticum)溶组织芽胞胶原酵素
http://www.aaos.org/news/aaosnow/oct10/clinical2.asp
发自我的 iPhone
我观察Dr.Eaton两年多了。也许有一天会在美国见到他。



发自我的 iPhone
我观察Dr.Eaton两年多了。也许有一天会在美国见到他。
8 days after treatment for Dupuytren contracture in the first metacarpophalangeal (MP) joint of the ring finger

(different patient) 1 month after injection to ring MP and before injection to middle MP

(same patient) 2 months after injection to ring MP and 1 month after injection to middle MP.

New treatments for Dupuytren contracture
D. Kay Kirkpatrick, MD, leads a roundtable discussion
Recently, the U.S. Food and Drug Administration (FDA) approved a new treatment for Dupuytren contracture—an enzyme injection (collagenase clostridium histolyticum) to soften and weaken the diseased cords of tissue that cause fingers to contract. In addition, other treatment options such as needle aponeurotomy—a minimally invasive technique that uses needles to puncture and weaken the contracting cords until they can be broken by mechanical force—are providing alternatives to surgery.
D. Kay Kirkpatrick, MD, a hand surgeon and member of the AAOS Practice Management Committee, recently conducted a roundtable discussion on these new treatments. Joining her were Charles Eaton, MD, FACS; F. Thomas D. Kaplan, MD; and Roy A. Meals, MD.
D. Kay Kirkpatrick, MD | Roy A. Meals, MD |
F. Thomas D. Kaplan, MD | Charles Eaton, MD, FACS |
Dr. Kirkpatrick: Why do you think there is suddenly so much interest in new treatments when open fasciectomy has been the gold standard for so many years?
Dr. Meals: I think it’s just coincidental. Needle aponeurotomy was initially popular with rheumatologists in France, and only recently has it been practiced in the United States. Similarly, collagenase injections (Xiaflex, Auxilium Pharmaceuticals, Inc., Malvern, Pa.) have been in clinical trials for some time, but received approval from the FDA just this year.
Dr. Eaton: I think it started with a combination of patients, surgeons, and the Internet as a vehicle for communication. The unmoderated online BioSpecifics Dupuytren patient discussion group enabled patients to spread the word about needle aponeurotomies. Patients then tried to recruit U.S. surgeons to provide this treatment. When I learned the technique, I was overwhelmed by patients who found me online.
Dr. Meals: The general trend is toward minimally invasive surgery.
Dr. Kirkpatrick: Let’s move on to collagenase injections. What are the clinical indications? What are—or are there—advantages in using collagenase injections over needle aponeurotomy?
Dr. Kaplan: I think that the advantages of collagenase injections versus aponeurotomy are yet to be fully elucidated. So far, collagenase injections have only been looked at on their own compared to placebo injections. Aponeurotomy has been looked at and compared to total or limited fasciectomy, but collagenase injections haven’t really been compared to needle aponeurotomy. That research still needs to happen.
Based on Phase I clinical trials, collagenase injections work better for metacarpophalangeal (MP) joint contractures than for proximal interphalangeal (PIP) joint contractures, and for lower severity contractures than for higher severity contractures.
Ideally, patients for collagenase injection should have a well-defined, palpable cord, ideally one that is strung away from the flexor tendon system. The worst patient is probably someone who has a small finger IP contracture that’s more than 50 degrees and has been there for 5 or 10 years. Collagenase can only affect the cord itself; it won’t be able to act on the secondary tissues that have changed.
Dr. Meals: One other consideration is that the collagenase injection requires two office visits—the injection on day one, and the manipulation of the finger to rupture the cord on day two. Some surgeons can perform needle aponeurotomy in their offices, but in California, the Medicare carrier will not pay for needle aponeurotomy in a nonfacility setting. That means a trip to a minor operating room, with all the associated facility and cost issues.
Dr. Eaton: I think that the primary advantage of the collagenase treatment is that it does not have as much of a learning curve as a percutaneous needle release. It is technically simple to perform, relatively quick, and much less demanding. Giving a shot is fast, but performing a needle aponeurotomy may take up to 20 minutes, depending on the severity. If multiple fingers are involved, the procedure may take closer to an hour. That can be an ordeal for the patient.
Dr. Kirkpatrick: What about the risks of these two procedures?
Dr. Meals: Each of these treatments has its own risk profile, different from the other. Needle aponeurotomy would be risky for the digital nerves, which the collagenase injection typically does not put at risk. On the other hand, two patients in the clinical trials did have tendon ruptures following collagenase injections.
Dr. Kaplan: Tendon rupture is also a risk of needle aponeurotomy. Another issue to consider with collagenase is that you can only inject one cord for one joint at a time, and injections must be at least a month apart because that’s the way it was tested. We don’t know whether giving two injections at the same time—even if in different hands—will result in worse side effects or an immunologic response.
Needle aponeurotomy can be used to treat multiple affected fingers and joints during one setting. We need to keep these parameters in mind when selecting what may be the best procedure.
Dr. Eaton: The other issue is what happens when someone has a recurrence after receiving treatment. Early on, there was concern that the collagenase would cause a gross architectural change and make surgical exploration difficult. But the few reports of patients who have had recurrences after an initial collagenase injection have been very favorable.
In contrast, the scar tissue that forms after needle aponeurotomy can be extensive and I suspect may be closer to the kind of scar tissue that forms after a fasciectomy. That in itself may be a long-term advantage in terms of the recurrence timeline between the two procedures.
Dr. Kirkpatrick: Are the contraindications for needle aponeurotomy and collagenase injections the same or different?
Dr. Eaton: Collagenase is contraindicated for patients who are on anticoagulation, but that is not an issue for needle aponeurotomy because the skin stops bleeding quickly after a puncture wound. Another potential limitation for collagenase would be lymphedema or prior lymph node surgery on the side being treated. A percentage of people will have a lymphatic reaction after collagenase injection. The only other issue is a patient who had previous surgery and has implants in that hand.
Dr. Kaplan: Anticoagulation is not actually listed as a contraindication for collagenase injection, but is a precaution. In the clinical trial, patients were excluded if on anticoagulants other than low-dose aspirin. We don’t know if this will be an issue or not, but we do ask patients who are on anticoagulation drugs to stop for 5 days before receiving collagenase injections.
Dr. Kirkpatrick: What do you think the role of open surgery is? Is it still the gold standard or the procedure of choice?
Dr. Meals: When open surgery is done properly and the patient sees it through with therapy, the likelihood for a functionally significant recurrence of the contracture is small. Unless the contracture has a real tendency to re-form, the chances are that the patient will not need any additional treatment in that area.
Based on reported results, recurrence within several years can be expected with needle aponeurotomy. The recurrence rate on the collagenase injection is unknown. Some people prefer to have a procedure done in the office rather than in an operating room; others would prefer to have one treatment now and stay out of doctors’ offices for a long time. Open surgery clearly has a role, even in previously untreated Dupuytren.
Dr. Kaplan: We really have to change our mindsets. This disease does not have a cure; what we do is manage the patient’s disability and impairment as best as we can. The best treatment depends on the patient—what the risk factors are for recurrence, how many joints are affected, age, and tolerance for open surgery versus a more percutaneous or limited approach.
I would like to make one other observation. A patient who has three or four contracted joints, with one finger particularly contracted, may be happy with having the collagenase injection in that finger to let it extend as much as the adjacent fingers. This limits, but does not eliminate, the disability. A limited approach in some patients may actually allow them to recover full function without aiming for the goal of getting full extension.
Dr. Kirkpatrick: The cost of the collagenase injection has been a huge issue in my practice. Carriers don’t seem to be routinely paying for this drug, and Medicare doesn’t have a specific code. Does anybody have a solution for that yet?
Dr. Meals: As of today in Southern California, Medicare is reimbursing collagenase injections and allowing the 6 percent markup to the surgeon. In preferred provider organizations when the insurance company approves it, the company contracts with a specialty pharmacy, which delivers the drug for those insured patients. I’m reimbursed for the procedure without being involved in the purchase of the enzyme itself.
Dr. Kaplan: As far as commercial payors, several have approved collagenase injections for patients, but one still considers it experimental.
Dr. Kirkpatrick: A lot of people are waiting to see what develops. The marketing of this product has been fairly aggressive. Does anyone have any issues with that?
Dr. Kaplan: I attended the FDA panel review, along with several hand surgeons and rheumatologists. Interestingly, the hand surgeons were more open to allowing non–hand to surgeons administer the collagenase injections than the rheumatologists were. The FDA clearly stated that it did not want to be overly restrictive or limit patient access.
I think the most important issue with the use of this product is that you be familiar with the anatomy of Dupuytren disease, regardless of whether you are a rheumatologist, orthopaedic hand surgeon, or plastic hand surgeon.
Dr. Kirkpatrick: Are you aware of other new treatments under development that have potential in this area?
Dr. Eaton: At an international symposium on Dupuytren disease in Miami earlier this year, we had 47 speakers from 13 different countries with some very interesting information and some new ideas. These included the use of custom silicone rubber splints after surgery that showed progressive improvement and extension over the course of months.
A report on using an absorbable carboxy cellulose implant as a spacer at the end of a limited fasciectomy for Dupuytren showed better early term results than not using that type of spacer. A variation of a needle release technique, using multiple superficial releases of the fascia over the entire distance of the palm, was also reported.
The most groundbreaking presentation was on the use of preoperative adjuvant tamoxifen to treat patients who had high risk for recurrence after a surgery. This randomized study showed that high-risk patients who had the preoperative treatment before limited fasciectomy for Dupuytren maintained their surgical correction to within about 10 degrees. Patients who were randomized to just the surgical treatment lost an average of 40 degrees of their initial correction.
The study used oral tamoxifen, but I’m considering a trial with topical tamoxifen. The big issues with patients who have aggressive Dupuytren are the extent of skin involvement and the dense relationship between the skin and the fascia as part of the biology. A minimal approach to straighten the fingers, followed by some sort of biologic intervention to maintain those results, would be great.
Radiation has been a commonly used approach in Germany. Radiation does have a biologic effect on nodular Dupuytren but not on the cords; it’s an option for patients who have early Dupuytren with a lot of nodular involvement. The amount of radiation used in the current protocols is fairly low and the chance of side effects is low, but we have yet to see long-term results.
Dr. Kirkpatrick: I think you have done a great job in bringing us up-to-date on what’s really going on, even though we may still have questions about how the various modalities are going to fit into our individual practices. Do you have any final comments?
Dr. Eaton: We need to organize large-scale studies to really look at our results. That’s the only way we will continue to make progress.
Dr. Kaplan: I want to echo those remarks. It’s so difficult to sort out the different techniques of needle aponeurotomy, fasciectomy, definitions of recurrent or disease extension, and patients’ different biology and risk. We need multicenter prospective trials with large numbers of patients to compare all these treatment options so we can make the best decisions.
Disclosure information: Dr. Kirkpatrick—no conflicts; Dr. Eaton—no conflicts; Dr. Kap-lan—Auxilium Pharmaceuticals; Acumed, LLC; Dr. Meals—Auxilium Pharmaceuticals, George Tiemann and Company, Hely-Weber.
AAOS Now
October 2010 Issue
http://www.aaos.org/news/aaosnow/oct10/clinical2.asp
October 2010 Issue
http://www.aaos.org/news/aaosnow/oct10/clinical2.asp
Samstag, Oktober 23, 2010
Sonntag, Oktober 17, 2010
Samstag, Oktober 16, 2010
Freitag, Oktober 15, 2010
Mittwoch, Oktober 13, 2010
"观于海者难为水,游于圣人之门者难为言"
今天下午,疼痛讨论会。
那些家庭医生不是一般的难对付。
介绍了两个病人,
一个是腰椎手术后综合症,我们治疗后不用服鸦片类止痛药了,随访了4年。
一个是紧张性头痛的患者,今年3月治疗,5年的头痛,一次治疗,不再复发。随访了7个月。
发自我的 iPhone
那些家庭医生不是一般的难对付。
介绍了两个病人,
一个是腰椎手术后综合症,我们治疗后不用服鸦片类止痛药了,随访了4年。
一个是紧张性头痛的患者,今年3月治疗,5年的头痛,一次治疗,不再复发。随访了7个月。
发自我的 iPhone
Dienstag, Oktober 12, 2010
FOCUS Online: Eine Schachtel kostet bis zu 107 Euro
Aus der FOCUS-Online-iPhone-App:
Rauchen - Eine Schachtel kostet bis zu 107 Euro
http://tinyurl.com/363df9x/?mobile=no
Von meinem iPhone gesendet
Montag, Oktober 11, 2010
Freitag, Oktober 08, 2010
FOCUS Online: Elektrische Entladungen im Gehirn
Aus der FOCUS-Online-iPhone-App:
Epilepsie - Elektrische Entladungen im Gehirn
http://tinyurl.com/247qlx5/?mobile=no
Von meinem iPhone gesendet
Donnerstag, Oktober 07, 2010
stern.de: Kinderkrankheit Rückenschmerzen
Aus der stern.de-iPhone-App:
Krankenkassen-Studie - Kinderkrankheit Rückenschmerzen
Link zum AppStore: http://itunes.apple.com/de/app/stern-de/id306192028?mt=8
Von meinem iPhone gesendet
Dienstag, Oktober 05, 2010
stern.de: Die Kleinen besiegen die Großen 电子阅读器比较
Aus der stern.de-iPhone-App:
E-Book-Reader im Test - Die Kleinen besiegen die Großen
Link zum AppStore: http://itunes.apple.com/de/app/stern-de/id306192028?mt=8
Von meinem iPhone gesendet
Sonntag, Oktober 03, 2010
stern.de: Die verwirrende Vielfalt der App-Stores
Aus der stern.de-iPhone-App:
Smartphone-Helferlein - Die verwirrende Vielfalt der App-Stores
Link zum AppStore: http://itunes.apple.com/de/app/stern-de/id306192028?mt=8
Von meinem iPhone gesendet
Samstag, Oktober 02, 2010
明天德国重新统一20年
柏林墙倒塌
20年庆典前,今年在不来梅,中国确实不应该一直在北京
三个城市
20年前后对照
2010.10.3
Der Islam gehört zu Deutschland,总统讲话
BERLIN - DAMALS UND HEUTE,柏林今昔
Prager Botschaft,前西德住捷克大使馆,除柏林墙,这里也值得纪念
Deutschland-von-A-bis-Z
20年庆典前,今年在不来梅,中国确实不应该一直在北京
三个城市
20年前后对照
2010.10.3
Der Islam gehört zu Deutschland,总统讲话
BERLIN - DAMALS UND HEUTE,柏林今昔
Prager Botschaft,前西德住捷克大使馆,除柏林墙,这里也值得纪念
Deutschland-von-A-bis-Z